How health technology is replacing care with surveillance
Surveillance technology in health and social care like Oxevision is intrusive, coercive and not fit for purpose, and much of its development links to warfare. Why is it being commissioned, and where could we find alternatives?

Hello! My name is Blue and I’m working with GFSC as an intern over the summer. In this blog I’ll talk about how technology is used in health and social care, why that’s a problem and how approaches led by GFSC such as community technology partnership can make a difference. The internship is funded by the Digital Good Network – a research network that focuses on “what a good digital society should look like and how we get there”.
The problem with technology in health and social care
Last year, a public inquiry started hearing evidence about 2,000 deaths of patients in mental health services at the Essex Partnership University NHS Foundation Trust. Key to the investigation is the use of one specific technology called Oxevision. Used across roughly 40% of NHS Trusts inside inpatients’ bedrooms, this technology is use for “remote monitoring” – aka surveillance – by staff in inpatient wards. The campaign group Stop Oxevision has worked tirelessly to research and collect testimonies. Here are examples of what people said to them:
It felt like staff would be sat in the office with a bucket of popcorn watching all the patients like a human zoo. [1]
There was an Oxevision device on the ceiling in the corner of the room that I hadn’t noticed. I felt humiliated to realise staff had been watching me. Had I been picking my nose? Had I masturbated? Had I got undressed within sight of the camera? I couldn’t remember and didn’t know what they might have seen. It was so humiliating. [2]
As a male staff member it was uncomfortable being asked to check the cameras to see what a patient was ‘up to’. [3]
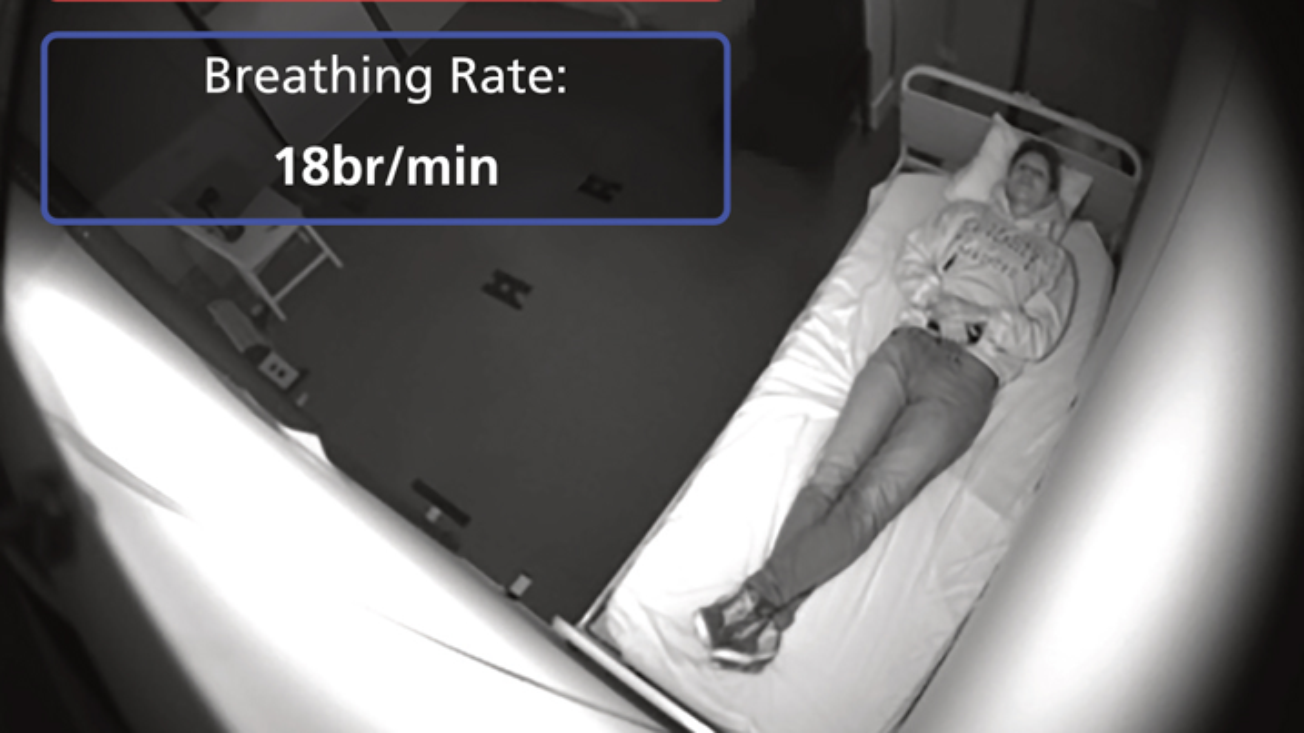
Originally developed at the University of Oxford and now commercialised through a spin off company called LIO (formerly Oxehealth), Oxevision is an infrared camera and sensors, mounted in a box in the ceiling of patients' bedrooms. It is connected to a software in the staff office in the ward as well as to an app on tablets used by staff. The camera and sensors collect data which is analysed by the software, which in turn issues alerts that staff in theory attend to. The software is supposedly used by staff to remotely view a patient in their bedroom and get a breathing and pulse reading to make sure they’re physically OK. Suddenly the nursing station in the ward has been turned into the security desk CCTV feed in a supermarket, and nurses have been turned into security guards.
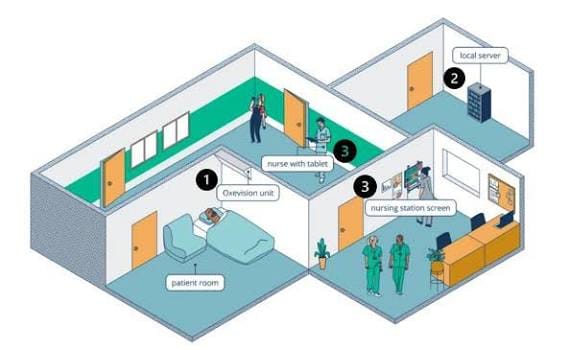

On the left: how Oxevision works across the ward. On the Right: What Oxevision camera and sensors look like
Oxevision is wrong for so many reasons. Patients have described it as creepy and unsafe, and many of the people I interview and speak to in my research have described ways in which it has made them feel worse. On a practical level it doesn’t seem to work because taking a breathing or pulse reading requires people to be still and have enough skin exposed. In the public enquiry, counsel reviewed evidence of staff attempting to get a reading several times until giving up and carrying out the check in person instead. Staff have also reported alarm fatigue, meaning they might skip alarms displayed by the software. There’s also evidence that alarms might not be raised when they should, leading to increased harm and to avoidable and heartbreaking death.
The company LIO says the technology is not supposed to replace the in-person checks carried out on the ward (also known as clinical observations), but in practice that is what happens. In part this is also due to lack of staff: there’s a really high turnover rate on inpatient wards and the job is continuously devalued. Worse, one of the justifications for using the technology in the first place is that it would save NHS Trusts money by reducing incidents and the need for bank staff.
How did we get here?
You may have noticed that accessing health and social care services is increasingly mediated by some kind of technology. For example, you may have been referred to a CBT courses that requires you to log in to an online platform, been referred to a private provider for an ADHD or Autism diagnosis and have to report symptoms and progress via their custom online platform, or an older person in your community may have been given various gadgets to manage fall risks at home. There’s also the very public case of private companies contracted by the NHS to ‘federate’ many different datasets – except the private company in question, Palantir, was able to get this analytical capacity by letting their systems learn in the context of war and genocide in Palestine.
This push towards digital and datafied services is clearly laid out in national policy: in the government's 10-year plan for health the key priorities are community, prevention and data. What this means is that there’s a strong emphasis on transforming services from analogue to digital. The narrative is that by collecting and analysing data, and training technology on it, services can be improved and people who use said services will experience better care outcomes. For example, it is often said that if all services have access to the same information then they make fewer mistakes and patients benefit from not having to explain their needs over and over again. So far so good. Unfortunately what this policy really translates to is a gold rush for the private sector to extract and exploit public health data in the community, in hospitals and in people’s homes.
Make no mistake, this kind of technology comes from warfare, intelligence and the criminal justice system and so when it spreads across society it brings increased securitisation and coercion with it. It’s not random that technology designed to extract, analyse or learn from data is introduced in settings where there’s already existing coercive practices. And when it does we can see the violence increase with unprecedented scale. In fact, there's a long and little heard history between the development of technology to be used by or on disabled people and warfare.
Of course, digital health is nothing new. As with every other corner of society, the health and care sector is increasingly datafied and digitalised and so-called ‘solutions’ are driven by a combination of publicly funded research and the private sector. Both Palantir and LIO/Oxehealth are spin-offs from publicly funded institutions. The technology itself is a problem, but it’s also thanks to a complex layer of governance that the way we use technology in health and social care is possible. In the case of Oxevision or Palantir's contract, decision-making comes from higher up so we can only fight back with national campaigning. However, I do believe that we can achieve change by addressing how decisions about technology are made at a more localised level.
Specifically, the way technology finds its way to health and care services in the community is through something called ‘commissioning’. I believe that a large part of the issue with the technology we find in health and social care can be addressed at the procurement level. In simple terms, commissioning is the process of selecting health and care solutions from an internal market where service providers are competing against each other. It came about with reforms in the 1990s that separated purchasing and delivering services. This clearly laid the foundation for the situation we find ourselves in today where across all levels of care, solutions are sought from a competing pool of providers, and increasingly private ones. One side effect is a massive leak of public funding to the private sector.
Why the technology community partnership approach could make a difference
My research is focused on increased securitisation, criminalisation and coercion such as surveillance technology in inpatient mental health care. I got into this because I was concerned about what happens to care outcomes when we collect data, use it to predict a risk and make decisions about a patient based on this information. I’ve used mental health services since I was a kid so this is something I feel quite concerned about.
When I came across the Digital Good Network’s funding for internships it felt like a great opportunity to work with GFSC. I was getting towards the end of the first year of my PhD and I was experiencing a lot of fatigue over my topic. Very little research was giving me any kind of confidence about how technology gets developed and commissioned, specifically to address social issues.
In the past I experienced technology as something that could be fun and emancipatory, for example I made music using live coding tools for a while and found it incredibly liberating. But now I feel there is no other choice but to argue for less technology because I believe it leads to better outcomes for social issues. Call me a luddite!

Reading Kim and Stefan White’s article on the PlaceCal pilot finally gave me hope for a path forward, because I felt it was addressing the problems I kept witnessing. The paper laid out a clear plan for action at a community level, naming technosolutionism as the problem. I immediately thought: with the community technology partnership approach (CTP), commissioners wouldn't have to buy ready-made products and hope that their community might adapt to it. Instead, they could address social problems by first looking at how people are already organising themselves and finding out what they actually need to improve problems they're facing.
I also believe there’s a strong health economics argument for a CTP approach, mainly because there’s a lot of waste when things aren’t a good contextualised fit. With this approach, technology providers aren’t considered to have a track record simply because of the scale of their activity and size. Instead, a CTP approach searches for a genuinely socially valuable output, not a manufactured and doubtful ‘evidence-based’ interventions. This holds technology tied to military intelligence and warfare at bay, because the quality of the technology in a CTP is determined by what it can do to support specific needs in a specific groups of people.
In the face of increased securitisation, coercion and criminalisation, it’s clear to me that data justice is disability justice and vice versa. My main motivation is to try to protect people from the harm associated with increased coercion and surveillance. So my plan for this internship is to help GFSC develop consulting materials to start advising the health and social care sector on alternatives. You may have followed GFSC’s plan to develop new funding streams including consultancy.
We need to fight back, and I believe it can start with influencing how technology is introduced locally though commissioning.


Comments ()